
What is Chronic Venous Disease/Insufficiency (CVI)?
What is Chronic Venous Disease/Insufficiency (CVI)?
The Macrovascular Root Cause: Chronic venous disease (CVD) is a highly prevalent, progressive condition affecting approximately 20% to 40% of the adult population in the United States alone. This long-term condition occurs when the internal, one-way valves inside the lower extremity veins become weakened, scarred, or incompetent. Normally, these valves keep blood flowing upward against gravity. When they fail, blood flows backward (refluxes) and pools in the legs, causing the internal pressure within the venous system to rise—a clinical state known as venous hypertension.
Why It Happens
Over time, several interconnected systemic and mechanical stressors damage the delicate vein walls and destroy valve utility:
- Genetic & Demographic Triggers: A known family history indicates a strong hereditary tendency, while advancing age significantly increases risk as vein walls naturally lose elasticity.
- Hormonal & Volumetric Stress: Pregnancy introduces elevated blood volume and profound hormonal shifts that place extreme structural stress on the venous walls.
- Mechanical & Lifestyle Demands: Prolonged standing or sitting forces the vascular system to work continuously against gravity without muscular assistance, while obesity directly increases intra-abdominal pressure, restricting efficient blood return.
- Thrombotic Damage: Prior episodes of Deep Vein Thrombosis (DVT) pose a severe threat, as active blood clots can permanently scar the vein walls and completely obliterate valve functionality.
What It Looks and Feels Like
The progression of chronic venous insufficiency develops slowly and is graded by clinicians on the standardized CEAP scale, ranging from C0 (no visible signs) to C6 (active, open skin ulceration):
- Early Stages (C1–C2): Begins as minor spider veins or small visible vessels on the skin surface, frequently progressing to prominent, swollen, and twisted varicose veins that bulge under the skin.
- Physical Sensations: Patients report profound leg heaviness, aching, throbbing, or a deep fatigue that worsens significantly after prolonged periods of standing.
- Advanced Tissue Damage (C3–C6): Chronic fluid pooling manifests as severe swelling (edema) of the ankles and lower legs. Left unmanaged, the fluid overload causes severe skin alterations: darkening or hyperpigmentation around the ankles, dry and intensely itchy skin (stasis dermatitis), and a progressive thickening or hardening of the subcutaneous tissue.
- The Ultimate Breakdown (C6): The final stage results in open venous leg ulcers, typically located near the ankle. These wounds are exceptionally slow to heal; statistically, roughly 20% of these open sores remain entirely unhealed even after two years of traditional care.
How It Is Managed
Clinical management focuses intensively on reducing venous hypertension, restoring fluid dynamics, and preventing tissue breakdown:
- Medical-Grade Compression: Wearing specialized compression stockings is foundational; these garments squeeze the limbs externally to counteract venous pooling and assist in pushing stagnant blood upward. Normally 20-30mmHg is the minimal grade necessary to see a difference. Compression needs to be properly fitted and "medical grade". Recommended brands would be: Sigvaris, Jobst, Juzo, Medi.
- Gravitational Unloading: Elevating the lower extremities above heart level multiple times throughout the day utilizes gravity to drain pooled fluid out of the lower limbs.
- Activating the Muscle Pump: Dedicated walking routines and active calf-pump exercises force the lower leg muscles to contract, mechanically squeezing the deep veins to pump blood back toward the heart.
- Advanced & Surgical Interventions: For severe or highly progressive cases, modern medical procedures can completely close off or remove the damaged veins using minimally invasive techniques (such as radiofrequency ablation, endovenous lasers, or targeted injections) and traditional surgery.
References:
1.Nonsurgical Management of Chronic Venous Insufficiency.
The New England Journal of Medicine. 2024. Fukaya E, Kolluri R.
2.Physical Exercise for the Treatment of Non-Ulcerated Chronic Venous Insufficiency.The Cochrane Database of Systematic Reviews. 2023. Araujo DN, Ribeiro CT, Maciel AC, et al.
3.Phlebotonics for Venous Insufficiency.
The Cochrane Database of Systematic Reviews. 2020. Martinez-Zapata MJ, Vernooij RW, Simancas-Racines D,
Journal of Vascular Surgery. 2014. O'Donnell TF, Passman MA, Marston WA
5.CHIVA Method for the Treatment of Chronic Venous Insufficiency.
The Cochrane Database of Systematic Reviews. 2021. Bellmunt-Montoya S, Escribano JM, Pantoja Bustillos PE, Tello-Díaz C, Martinez-Zapata MJ.
6.ACR Appropriateness Criteria® Lower Extremity Chronic Venous Disease.Journal of the American College of Radiology : JACR. 2023. Rochon PJ, Reghunathan A, Kapoor BS
7.Balneotherapy for Chronic Venous Insufficiency.
The Cochrane Database of Systematic Reviews. 2023. de Moraes Silva MA, Nakano LC, Cisneros LL
8.Chronic Venous Disease. Part 1: Pathophysiology and Clinical Features.
Clinical and Experimental Dermatology. 2022. Kumar P, Khan IA, Das A, Shah H

What is Lower Leg Lymphedema (Phlebolymphedema)?
What is Lower Leg Lymphedema (Phlebolymphedema)?
The Microvascular Clearing Failure: Lymphedema is a chronic, progressive condition in which fluid builds up in the interstitial tissues of the leg because the lymphatic system can no longer drain it properly. Separate from veins and arteries, the lymphatic system acts as the body's essential drainage network, collecting excess fluid from the tissues and returning it safely to the bloodstream. When advanced chronic venous insufficiency (specifically stages C3 through C6) is the direct underlying driver of this drainage failure, the condition is clinically termed Phlebolymphedema—representing a dual-system collapse where vein ("phlebo") and lymphatic problems occur simultaneously. As leading vascular experts have established, advanced chronic venous insufficiency always manifests as a chronic venous-lymphatic insufficiency.
How Chronic Vein Disease Destroys Your Lymphatics
The venous and lymphatic systems are intimately connected and depend on each other to maintain fluid balance. When a patient experiences underlying venous disease, it triggers a step-by-step destruction of the local lymphatic channels:
- Step 1 — The Macrovascular Overload: As the one-way valves in the leg veins fail, blood pools in the lower limbs, driving internal venous hypertension straight through the roof.
- Step 2 — Interstitial Flooding: This intense back-pressure forces abnormally high volumes of fluid out of the tiny blood vessels and into the surrounding tissue spaces. At first, your lymphatic system attempts to compensate by working overtime to absorb and drain this massive influx.
- Step 3 — Systemic Overwhelmed Capacity: Over time, the sheer, unrelenting volume of fluid completely exceeds what the lymphatic vessels can physically handle—similar to a storm drain overflowing during a massive downpour.
- Step 4 — Permanent Structural Damage: If the root venous hypertension goes untreated, the constant fluid overload and chronic inflammation permanently destroy the lymphatic anatomy. The tiny lymphatic channels in the skin become blocked, their walls collapse, and the micro-anchoring structures holding them open are obliterated. At this point, the structural damage becomes difficult or impossible to reverse.
How Common Is It? (The Hidden Leading Cause)
Phlebolymphedema is far more common than most of the medical community realizes. An estimated 5 to 10 million people in the United States live with some form of lymphedema.
Remarkably, phlebolymphedema has emerged as the leading cause of lower extremity lymphedema cases—accounting for roughly 42% of all clinical cases in a landmark study, which actually exceeds cancer-related lymphedema (34%). Despite this massive footprint, it remains widely underdiagnosed and undertreated across standard primary care environments.
What It Looks and Feels Like: The Clinical Stages
Lower leg lymphedema progresses through four recognized, highly defined stages, transitioning from completely invisible to severe tissue alteration:
- Stage 0 (Subclinical/Hidden): The internal lymphatic system is already actively struggling, but there is no visible swelling yet. Patients typically report a subtle, deep heaviness or achiness in the leg. This latent stage can persist for months or even years before swelling physically manifests.
- Stage 1 (Early/Reversible): Visible swelling develops, peaking heavily by the end of the day. The swelling is soft and "pitting"—meaning if you press a finger into the skin, it leaves a distinct, temporary indentation. Crucially, at this stage, the swelling completely resolves or goes down with leg elevation after a night's rest.
- Stage 2 (Persistent/Irreversible): Swelling no longer goes away with elevation or rest. The tissue begins to feel firm and brawny as scar-like tissue (fibrosis) actively develops in the skin and subcutaneous fat layers, causing the skin to thicken.
- Stage 3 (Severe/Elephantiasis): The limb becomes massive, hard, and structurally disfigured. The skin thickens dramatically, developing deep folds, fatty tissue deposits, and warty bumps. Pressing on the skin no longer leaves an indentation because the underlying fibrotic tissue is entirely firm. At this final stage, the swelling is essentially permanent and exceptionally difficult to treat.
The True Dangers of Leaving Lymphedema Untreated
Ignoring progressive lower leg lymphedema carries severe, systemic health risks that extend far beyond cosmetics:
- Recurrent Skin Infections (Cellulitis): Stagnant, protein-rich interstitial fluid serves as an ideal breeding ground for bacteria. Repeated bouts of cellulitis are incredibly dangerous, and each subsequent infection further scars the remaining lymphatic vessels, trapping the patient in a vicious biological cycle.
- Skin Breakdown & Lymphorrhea: The skin becomes intensely fragile, dry, and prone to cracking, fungal infections, and open leaking of fluid through the skin surface (lymphorrhea).
- Loss of Mobility & Muscle Atrophy: A heavy, swollen limb makes normal walking difficult. This forced immobility directly weakens the calf muscles—the precise muscular pump needed to mechanically drive fluid back up the leg—worsening the entire condition.
- Malignancy Risk (Rare but Lethal): In very long-standing, severe, unmanaged cases, a rare and highly aggressive vascular cancer called lymphangiosarcoma can develop directly within the chronic lymphedematous tissue.
How Phlebolymphedema Is Expertly Managed
While there is no cure for permanent lymphatic failure, professional management can successfully halt disease progression, reduce limb volume, and prevent critical complications.
- Target the Venous Driver First: Since chronic venous disease is the underlying catalyst, correcting the macrovascular venous hypertension through medical-grade compression or minimally invasive vascular procedures is an essential first step that can directly improve lymphatic efficiency.
- The Gold Standard: Complex Decongestive Therapy (CDT): This specialized, physical therapy framework is executed in two strict phases:
- Phase 1 (Intensive Reduction): A certified lymphedema therapist (CLT) performs Manual Lymphatic Drainage (MLD) to gently redirect trapped fluid into working channels, applies specialized multi-layer compression bandages, guides decongestive exercise, and establishes meticulous skin care.
- Phase 2 (Home Maintenance): The patient transitions to long-term independent care, utilizing custom-fitted daytime compression garments, self-massage protocols, regular exercise, and absolute skin hygiene.
- Consistent Compression Therapy: Ongoing compression wraps or stockings are the single most important tool to mechanically prevent fluid from pooling back down the leg.
- Advanced Pneumatic Compression Devices: Utilizing specialized at-home multi-chamber pumps (like the Flexitouch system) provides sequential, automated pulsing that moves fluid upward. Advanced devices are clinically proven to drastically cut hospital re-admissions and skin infections for phlebolymphedema patients.
- Activating the Calf-Muscle Pump: Structured walking and targeted exercises force active muscle contractions that pump both blood and lymph back to the heart, proving safe and highly effective at all stages.
What is lipedema?
What is lipedema?
Lipedema (Disproportional Adipose Disorder)
The Adipose & Connective Tissue Enigma: Lipedema is a chronic, progressive disease of the loose connective and adipose tissue that results in a distinct, highly abnormal, and disproportionate bilateral accumulation of fat cells. Presenting almost exclusively in women, it primarily targets the lower extremities—specifically the hips, buttocks, and legs—and occasionally the upper arms.
Crucially, Lipedema is not simple obesity, nor is it lymphedema. This specific tissue is highly resistant to traditional metabolic interventions, meaning the characteristic lower-body disproportion persists entirely despite aggressive calorie restriction, intensive exercise regimens, or bariatric surgery. First clinically described in 1940, Lipedema remains one of the most widely misdiagnosed conditions in modern medicine, frequently written off as standard obesity or lifestyle non-compliance, leaving women stranded without answers or a diagnosis for decades.
Why It Happens (The Pathophysiological Catalyst)
While the precise cellular root cause of Lipedema is still undergoing rigorous investigation, clinical evidence points to a multi-systemic onset:
- Hormonal Triggers: Lipedema onset and progression are intimately linked to major endocrine shifts. The disease almost universally surfaces or flares during windows of significant hormonal volatility: puberty (accounting for roughly 62% of clinical presentations), pregnancy, or menopause, strongly indicating that female sex hormones (estrogen) act as a primary receptor trigger.
- Genetic Heredity: There is a profound inherited component to Lipedema architecture. Approximately 50% of women diagnosed with the condition have a documented female family member navigating the exact same physical traits, demonstrating a clear genetic lineage.
- Microvascular & Endothelial Dysfunction: Emerging vascular research reveals that the microcirculation feeding lipedematous fat is fundamentally fragile and leaky. This structural capillary permeability leads to micro-vascular fluid leakage into the interstitial spaces, fueling localized hypoxia, chronic low-grade tissue inflammation, and subsequent tissue swelling.
- The Venous Insufficiency Overlap: Macrovascular breakdown is heavily intertwined with this disorder. In a landmark retrospective study, a staggering 86% of lipedema patients presented with coexisting chronic venous disease, marking it as the single most common comorbidity. These two distinct vascular conditions frequently exacerbate one another, drastically accelerating lower limb tissue breakdown.
What It Looks and Feels Like: The Clinical Types & Stages
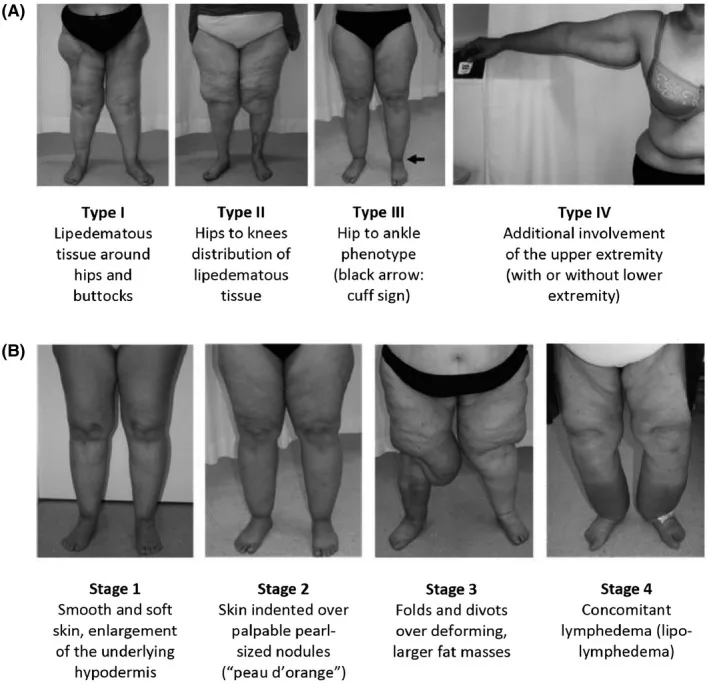
Lipedema is physically categorized by its structural distribution across five clinical Types (defining where the tissue accumulates) and graded across four distinct anatomical Stages (defining how the tissue alters skin and fat architecture):
The Anatomical Types (Distribution Pools)
- Type I: Adipose accumulation is concentrated strictly around the pelvis, buttocks, and hips.
- Type II: The tissue extends from the buttocks down the thighs, terminating sharply right at the knee margins.
- Type III: The most common presentation; tissue extends from the hips all the way down the leg, terminating in a distinct structural boundary right above the ankle joints.
- Type IV: The upper arms are heavily involved, presenting with a prominent tissue drop that stops abruptly at the wrists.
- Type V: The adipose tissue is isolated exclusively to the lower calves and ankles.
The Progressive Clinical Stages
- Stage 1: The skin surface remains entirely smooth and uniform. However, the subcutaneous fat layer is noticeably thickened, and manual palpation reveals an underlying tissue structure that feels like "small marbles" or soft pearls suspended beneath the skin.
- Stage 2: The skin surface begins to lose its uniformity, presenting an irregular, dimpled, or "mattress-like" texture. The subcutaneous architecture grows larger, and nodular masses can be easily felt upon palpation.
- Stage 3: Severe, structural deformity takes over the limb. Massive, overlapping lobes of fibrotic, hardened fat accumulate along the thighs, knees, and ankles. These heavy tissue folds distort normal walking mechanics, placing immense mechanical stress on the joints.
- Stage 4 (Lipo-lymphedema): The final phase of total fluid failure. The massive, long-standing adipose lobes and chronic microvascular fluid overload completely crush and exhaust the local lymphatic vessels. The lymphatic system fails permanently, superimposing secondary Lymphedema over the Lipedema, causing the feet to swell for the very first time.
Key Visual and Physical Identifiers (How to Tell the Difference)
To accurately differentiate Lipedema from standard obesity or primary lymphedema at the bedside, clinicians look for several hallmark diagnostic features:
- The Foot Sparing Test: A definitive diagnostic signature of Lipedema stages 1 through 3 is that the hands and feet are completely spared. The painful fat accumulation stops abruptly at the wrist and ankle bones, creating a prominent, distinct visual "cuffing" or "bracelet" effect.
- Exquisite Hypersensitivity: Unlike normal fat tissue, lipedematous tissue is highly painful, tender to light pressure, and aches continuously.
- Capillary Fragility: Because the tiny blood vessels within the tissue are structurally compromised, patients present with a history of spontaneous, easy bruising from minimal or unnoticed contact.
- Perfect Bilateral Symmetry: Lymphedema is overwhelmingly asymmetric (one leg is drastically larger than the other). Lipedema is strictly symmetric; both legs present identical, mirrored proportions, contours, and fat distribution from side to side.
Clinical Management of a Metabolically Resistant Disease
Because Lipedema fat entirely resists standard diet and weight loss medications, management shifts away from traditional caloric restriction and focuses heavily on tissue decompression, inflammation reduction, and surgical extraction:
- Rule Out Other Disorders First: Clear for concurrent venous disease, autoimmune disorder, pelvic vein compression, obesity or other etiologies. Encourage a vascular workup as part of the diagnosing process along with metabolic and hormone panel.
- Complete Decongestive Therapy (CDT): Utilizing gentle manual lymphatic drainage and specialized, flat-knit compression garments works to control interstitial fluid dynamics, soothe neuro-inflammation, and support microvascular return.
- The Anti-Inflammatory Framework: Management protocols lean heavily into specialized nutritional strategies (such as the RAD or ketogenic diets) designed explicitly to lower systemic inflammation, combined with low-impact movement mechanics (like aquatic therapy or structured strength training) to optimize the calf-muscle pump without inducing joint stress.
- *Last Resort*Advanced Liposuction (Surgical Extraction): For progressive or highly symptomatic cases, specialized Vaser or Water-Assisted Liposuction (WAL) is highly effective. Unlike cosmetic liposuction, medical lipedema surgery utilizes specialized blunt cannulas to meticulously protect the underlying lymphatic vessels while systematically debulking the painful, non-metabolic fat cells to restore mobility and permanently alleviate pain.
For further information please visit the Lipedema Foundation and review the work of Dr. Karen Herbst, MD
1. Standard of Care for Lipedema in the United States (Herbst et al., 2021) — This is the foundational U.S. consensus guideline on lipedema, developed using the Delphi Method with 85 consensus statements rated by the GRADE system. It defines lipedema as a "loose connective tissue disease" characterized by nodular and fibrotic adipose tissue on the buttocks, hips, and limbs, developing during hormonal transitions (puberty, pregnancy, menopause). It identifies key comorbidities including obesity, lymphedema, venous disease, and hypermobile joints, and provides medical, surgical, vascular, and therapeutic recommendations. [1]
2. Lipedema: Friend and Foe (Torre, Wadeea, Rosas & Herbst, 2018) — This paper uniquely examines both the harmful and potentially protective aspects of lipedema fat. It demonstrated that despite an average obese BMI of 35.3, lipedema patients had remarkably low rates of diabetes (2%), dyslipidemia (11.7%), and hypertension (13%) — suggesting that gynoid (hip/thigh) fat distribution may be metabolically protective. The study also found that 58% of lipedema patients had joint hypermobility, significantly higher than in Dercum's disease (23%), establishing hypermobility as a likely comorbid condition. [2]
3. Differentiating Lipedema and Dercum's Disease (Beltran & Herbst, 2017) — A case series of 94 patients with Dercum's disease and 160 with lipedema from Dr. Herbst's clinic, providing the first systematic comparison between these two frequently confused painful fat disorders. Key differentiating features included: lipedema patients had greater BMI, more gynoid fat distribution, more easy bruising, and significantly higher hypermobility (58% vs. 23%), while Dercum's disease patients had higher pain scores, more diabetes (16% vs. 6%), and more lipomas, fibromyalgia, and migraines. [3]
4. Lymphatic Function and Anatomy in Early Stages of Lipedema (Rasmussen, Aldrich, Fife, Herbst & Sevick-Muraca, 2022) — A landmark pilot study using near-infrared fluorescence lymphatic imaging in 20 patients with Stage I or II lipedema. The critical finding was that while lower extremity lymphatic vessels were dilated and showed intravascular pooling, propulsion rates actually exceeded those of controls, and there was no dermal backflow — in stark contrast to lymphedema. This provided direct evidence that lipedema and lymphedema have fundamentally different etiologies, despite their superficial clinical resemblance. [4]
5. Defining Lipedema's Molecular Hallmarks by Multi-Omics Approach (Straub, Funcke, Joffin, ... Herbst, Scherer, 2025) — A cutting-edge multi-omics study (transcriptomics, proteomics, metabolomics, lipidomics) that identified molecular signatures of lipedema, including adipokine dysregulation, downregulation of inflammatory factors, upregulation of mitochondrial/oxidative phosphorylation pathways, and altered sphingolipid and glutathione metabolism. The study also developed a serum-based predictive model for lipedema diagnosis — a potential step toward the first objective biomarker. [5]
6. Lipedema World Alliance Delphi Consensus (Kruppa, Crescenzi, ... Herbst, et al., 2026) — The most recent international consensus, published in Nature Communications, with experts from 19 countries (including Dr. Herbst). It achieved consensus on 59 statements across eight domains covering the definition and management of lipedema, providing a framework for internationally applicable recommendations. [6]
Additional Key References by Topic
Pathophysiology and Tissue Biology
- Cifarelli (2025) — A comprehensive systematic review of lipedema pathophysiology covering genetic predisposition, hormonal influences, vascular dysfunction, and the molecular differences between lipedema fat and obesity fat. [7]
- Kruppa et al. (2023) — Demonstrated stage-dependent adipocyte hypertrophy, progressive interstitial fibrosis, and elevated M2-like (anti-inflammatory) macrophage polarization in lipedema tissue — a pattern distinct from the pro-inflammatory M1 response seen in obesity. [8]
- Al-Ghadban, Guo, Juskiewicz, et al. (2026) — Detailed the vascular changes in lipedema including endothelial dysfunction, aberrant angiogenesis, vessel fragility, and the interplay between vascular, lymphatic, and immune dysfunction. [9]
- Rabiee (2025) — A review proposing that lipedema may represent a model of "healthy" subcutaneous adipose tissue expansion with preserved metabolic function, and suggesting menopause as a critical turning point driven by estrogen receptor imbalance. [10]
Diagnosis and Classification
- Kruppa et al. (2020) — A comprehensive review of lipedema pathogenesis, diagnosis, and treatment from the German literature, summarizing the clinical diagnostic approach and the lack of specific biomarkers. [11]
- Vazirnia et al. (2026) — The most recent systematic review of lipedema diagnosis and therapeutics, grading conservative therapies at Grade 2A-2B and tumescent liposuction as a Grade 1 recommendation. [12]
- van la Parra et al. (2024) — A systematic review of diagnostic imaging modalities for lipedema (ultrasound, lymphoscintigraphy, CT, MRI, DXA), concluding that diagnostic performance remains limited and prospective comparative studies are needed. [13]
Epidemiology and Clinical Characteristics
- Luta et al. (2025) — A large Swiss cohort (381 patients) showing that 86.2% had chronic venous disease, 51.7% had obesity, 87.9% had pain, and that age and BMI were independently correlated with advanced disease stage. [14]
- Buso et al. (2019) — "Lipedema: A Call to Action!" — a widely cited review calling attention to the underdiagnosis of lipedema and outlining its epidemiology, pathophysiology, and management. [15]
- Carballeira Braña & Poveda Castillo (2023) — A large Spanish cross-sectional study (1,069 patients) using Wolf's classification modified by Herbst, confirming that multidisciplinary management offers the best overall results. [16]
Surgical Treatment (Liposuction)
- Fijany et al. (2024) — The first meta-analysis comparing liposuction techniques (tumescent, power-assisted, water-jet-assisted) for lipedema across 2,542 procedures in 906 patients, showing significant symptom improvement with all techniques and low complication rates. [17]
- Hersant et al. (2026) — A large observational study of 191 patients undergoing ultrasound-assisted liposuction, demonstrating significant circumference reductions and pain improvement. [18]
- Karri (2025) — A UK longitudinal study showing significant improvement in health-related quality of life after liposuction, though scores did not fully normalize to population levels. [19]
Nutrition and Conservative Management
- Lundanes et al. (2024) — The first randomized controlled trial of a low-carbohydrate diet for lipedema, showing superior pain reduction compared to a standard calorie-restricted diet. [20]
- Atabilen Pınar et al. (2025) — A scoping review of nutritional approaches including ketogenic, low-carbohydrate, and modified Mediterranean diets, noting positive effects on body composition and pain but no evidence-based nutritional cure. [21]
- Keith et al. (2021) — A hypothesis paper exploring the mechanisms by which a ketogenic diet may alleviate lipedema symptoms through effects on inflammation, fibrosis, and adipose tissue metabolism. [22]
Lipedema and Connective Tissue / Hypermobility
- Fiengo & Sbarbati (2025) — A cross-sectional study finding that 44% of lipedema patients reported joint hypermobility and 60% recalled childhood hypermobility, with significantly more connective tissue-related symptoms than controls — supporting the concept of lipedema as a systemic connective tissue disorder. [23]

Other Sources of Edema
Other Sources of Edema
Post-Orthopedic Edema
The Traumatic Inflammatory Cascade: Post-orthopedic edema is an expected, acute consequence following bone fractures, joint injuries, or major surgical interventions (such as total knee arthroplasty, hip replacements, or complex hindfoot reconstructions). When bone, skin, and muscular tissue undergo direct surgical trauma, the body launches a highly localized inflammatory healing response. This response releases potent chemical markers that cause nearby microscopic blood vessels to become highly permeable or "leaky," flooding the surrounding tissue spaces with fluid, proteins, and immune cells to initiate tissue repair.
Why the Fluid Accumulates:
- Surgical Trauma & Hidden Blood Loss: The structural extent of the surgery directly dictates the swelling volume. Intravasation and hidden blood loss that seeps deeply into the surrounding soft tissues post-operatively serve as one of the single strongest predictors of extreme post-surgical swelling. Additionally, the use of a surgical tourniquet during the procedure further amplifies post-operative tissue engorgement.
- The Immobilization Trap: Following major bone or joint surgery, the limb is frequently immobilized in a rigid orthopedic boot, cast, or post-op splint. The human calf muscle pump normally acts as a mechanical engine, ejecting 100 to 150 ml of fluid upward with a single contraction during walking. When a surgical boot or splint completely stops ankle movement, this mechanical pump is neutralized, forcing fluid and blood to pool heavily in the dependent lower limb.
- The Latent Vein Disease Catalyst: Patients who present with underlying, pre-existing varicose veins or chronic venous insufficiency are at a vastly elevated risk for extreme, persistent post-operative leg swelling. A pre-operative great saphenous vein (GSV) diameter exceeding 5.5 mm serves as a powerful anatomical predictor of severe post-surgical fluid clearance failure.
Clinical Presentation & Timing:
Post-orthopedic swelling develops rapidly, typically reaching its absolute worst baseline between days 3 and 8 post-operatively, with peak volumetric expansion occurring at days 6 to 8. The operated limb swells disproportionately compared to the non-operated side, presenting as classic pitting edema. At its peak, the affected leg can measure 25% to 47% larger than its pre-surgical size. Tissues feel hot, taut, heavy, and structurally stiff, creating intense localized pain and significantly limiting knee or ankle range of motion.
- The Weight-Bearing Pivot: Clinicians and patients must recognize that a temporary, secondary wave of renewed swelling and pain frequently hits at exactly the 3-month mark following foot and ankle surgery. This is a recognized adaptation phase that triggers when patients transition back to full, unrestricted weight-bearing activities.
Clinical Management Protocols:
Management focuses on controlling localized inflammation, accelerating fluid clearance, and jumpstarting the calf-pump engine:
- Multilayer Compression Therapy: High-yield clinical trials demonstrate that applying multilayer compression bandages is significantly more effective than ice/cryotherapy alone. Multilayer compression reduces post-traumatic edema by 22% to 23% within 48 hours, compared to a meager 5% to 7% reduction achieved via ice application. Progress to 20-30 compression stockings.
- Gravitational Elevation & Positioning: Elevating the operated leg strictly above heart level utilizes gravity to drain pooled interstitial fluid out of the limb. For total knee replacements, maintaining the joint in 30° to 90° of flexion during the initial 6 to 72 hours post-op drastically curtails initial fluid buildup.
- Early Assisted Mobility: Implementing gentle, early physical therapy movement patterns restarts the calf muscle pump to clear protein-rich fluid before it hardens into fibrotic tissue.
- Pharmaceutical Interventions: Administering Tranexamic Acid (TXA) perioperatively stands as the most consistently effective systemic intervention for lowering post-operative swelling and hidden blood loss following total joint replacements.
🛑 When to Worry: While post-surgical swelling resolves gradually over several weeks, a sudden, asymmetrical worsening of swelling—especially if paired with acute calf tenderness, localized heat, redness, or sudden shortness of breath—demands immediate medical emergency evaluation to rule out a deep vein thrombosis (DVT).
Dependent Edema (Gravity-Related Fluid Pooling)
The Mechanical Transport Failure: Dependent edema is a purely gravity-driven fluid accumulation that targets the lowest, most gravity-dependent zones of the human body. In ambulatory individuals who spend their days upright, this manifest as bilateral lower extremity swelling around the feet, ankles, and calves. In patients who are bedridden or suffer from neurological conditions that keep them supine, gravity pulls this fluid backward, causing it to pool over the lower back (sacrum) and buttocks instead.
Why the Fluid Accumulates:
The vascular system continuously filters fluid out of the capillaries into the surrounding tissues, relying entirely on the lymphatic networks and venous system to reabsorb and clear it. To counteract the downward pull of gravity, the body depends on an active calf muscle pump, functional one-way venous valves, and continuous microvascular lymphatic drainage.
Dependent edema develops when these clearing mechanisms are entirely intact but are mechanically underutilized or overwhelmed by positional stagnation:
- Prolonged Occupational Stagnation: Extended periods of static sitting (desk work, long flights, wheelchair reliance) or prolonged stationary standing completely eliminates active calf muscle contractions.
- Immobility & Aging: Reduced physical mobility from aging, neurological deficits, or illness removes the mechanical pressure required to empty the lower extremity veins.
- Thermal Vasodilation: Hot weather acts as a physical trigger, forcing superficial blood vessels to dilate, which drastically increases microvascular fluid leakage into the skin tissues.
- Systemic Pathology Warnings: Crucially, persistent dependent edema can serve as an early clinical warning sign of life-threatening systemic organ failures—including congestive heart failure (volume overload), chronic kidney disease, or liver failure. It is also a notorious side effect of common neurological and cardiovascular medications, most notably calcium channel blockers (e.g., Amlodipine) and gabapentinoids.
Clinical Presentation & Timing:
Dependent edema presents with perfect bilateral symmetry, affecting both lower limbs identically. It follows a strict diurnal rhythm: it is virtually non-existent or mild in the morning, worsens progressively throughout the day as gravity acts on the limbs, peaks by the end of the evening, and completely resolves overnight when the patient sleeps flat, allowing gravity to distribute fluid evenly. The swelling is highly soft and pitting. It alters the feet and ankle contours first, slowly ascending up the calves only if the hydrostatic pressure remains unmanaged.
Clinical Management Protocols:
- Movement Over Medication: Walking, ankle pumps, and active physical therapy exercises are the simplest and most effective treatments, because turning on the calf pump immediately ejects stagnant blood out of the legs.
- Graduated Compression: Wearing 20–30 mmHg graduated compression stockings mechanically compresses the interstitial spaces, physically breaking up the gravity-driven fluid loop before the swelling can expand the tissue walls.
- Positional Elevation: Elevating the lower extremities above heart level multiple times a day forces gravity to work in reverse, draining the pooled volume toward the central circulation.
- Root-Cause Correction: If the fluid accumulation stems from heart or kidney dysfunction, treating the underlying pathology is mandatory. Systemic diuretics should only be utilized for true volume overload states (like heart failure); they are entirely inappropriate and clinically contraindicated for treating simple dependent edema or mechanical venous pooling.
Obesity-Related Edema
The Multi-Systemic Structural Blockade: Obesity-related edema is a chronic, progressive form of lower extremity swelling that develops as a direct physical and biological consequence of excess body mass. It stands as one of the most frequent yet underdiagnosed causes of chronic, bilateral lower limb swelling in primary care. As body mass index (BMI) climbs, it triggers a catastrophic multi-system overload that impairs both macrovascular venous return and microvascular lymphatic transport.
Why the Fluid Accumulates:
Obesity systematically destroys lower limb fluid equilibrium through a multi-layered cascade of mechanical and anatomical failures:
- The Abdominal "Dam" Effect: Excess intra-abdominal adipose tissue generates massive internal pressure, frequently rising from a normal status of under 5 mmHg to a highly pathologic 10 to 15 mmHg. This elevated pressure physically compresses the large deep veins within the pelvis (the inferior vena cava and iliac veins). This acts exactly like a structural dam, backing up blood flow and driving venous hypertension down into both legs.
- Secondary Venous Insufficiency: Chronically elevated venous back-pressure permanently stretches the leg veins, pulling the internal one-way valves apart and causing secondary chronic venous insufficiency. While lower limb venous disease affects up to 50% of the general population, its prevalence skyrockets inside the obese demographic.
- Direct Lymphatic Destruction: This is a critical, often-overlooked biological milestone. Excess weight directly damages the microvascular lymphatic architecture. Adipose expansion significantly reduces local lymphatic vessel density, destroys internal lymphatic valve utility, impairs active lymphatic pumping mechanisms, and causes the micro-vessels to become highly leaky. Clinical data proves that once a patient's BMI exceeds 40, the risk of permanent lymphatic system failure rises drastically; once BMI crosses 60, lymphatic dysfunction becomes nearly universal. This is known as OIL (Obesity Induced Lymphedema)
- Calf Pump Impairment: Elevated adipose mass surrounding the lower limbs combined with a sedentary lifestyle heavily restricts normal ankle mechanics, severely blunting the muscle pump's ability to clear fluid.
Clinical Presentation & Timing:
Obesity-related edema presents as a chronic, persistent, bilateral swelling that involves the entire lower leg, ankle, and crucially involves the feet.
- The Lipedema Distinction: Unlike Lipedema (which strictly spares the feet and stops at the ankle), obesity-related edema heavily affects the feet; the tops of the feet (dorsum) appear highly puffy, swollen, and pillowy.
In its earliest phases, the swelling is soft and pitting. However, as chronic fluid pooling transitions into permanent lymphatic failure, it evolves into a severe, irreversible state known as Obesity-Induced Lymphedema (OIL). At this juncture, the fluid becomes non-pitting, and the skin turns brawny, firm, and highly fibrotic. The leg displays the advanced tissue modifications of severe vein disease: rust-colored hemosiderin skin staining, stasis dermatitis rashes, and massive, overlapping folds of hardened skin that trap fluid and invite dangerous, recurring bacterial infections.
Clinical Management Protocols:
- Systemic Weight Loss: This is the most critical and fundamental treatment path. Weight loss stands as the only clinical intervention capable of reversing the underlying mechanical compression and biological lymphatic damage caused by excess mass. Metabolic surgeries (bariatric interventions) are clinically proven to immediately drop intra-abdominal pressure, reduce leg edema, and successfully close chronic, non-healing venous ulcers.
- Targeted Compression Therapy: Utilizing graduated compression stockings or multi-layer compression wraps is vital to counteract internal venous hypertension and support failing lymphatic drainage. Due to the physical contour changes of the limb, custom-designed or flat-knit compression garments are frequently required.
- Restoring Physical Activity: Implementing consistent, low-impact exercise routines (such as aquatic therapy or structured walking) immediately forces muscle contractions to assist the failing calf pump.
- Managing Co-Morbid Pressure: Obesity frequently coexists with obstructive sleep apnea (OSA), which causes a massive spike in central venous pressure that forces fluid downward. Consistently managing OSA with a CPAP machine reduces this central resistance, providing an essential decompression element to lower leg swelling.
- Eliminating Inappropriate Diuretics: Unless a patient has concurrent, documented systemic volume overload (such as from congestive heart failure), diuretics should be strictly avoided. Using diuretics for mechanical obesity-related edema or lymphatic clearing failure does not address the structural compression; instead, it risks causing severe systemic dehydration and critical electrolyte imbalances.
Evidence for 20–30 mmHg as the Appropriate Pressure
The 20–30 mmHg pressure range is well-supported for edema management in general with potential for post-TKA use:
- The Society for Vascular Surgery recommends 20–30 mmHg for varicose veins and edema, reserving 30–40 mmHg for venous ulcers. [8]
- An NEJM review on chronic venous insufficiency notes that while >30 mmHg is recommended for ulcer healing, 20–30 mmHg is often used as a balance between efficacy and adherence, since higher pressures significantly reduce compliance. [5]
- A meta-analysis of 11 RCTs found that compression needs to be at least 10–15 mmHg to be effective, but higher levels were not necessarily more beneficial — supporting the 20–30 mmHg range as a reasonable balance. [6]
- In stockings specifically, swelling reduction tends to positively correlate with volume reduction up to 30 mmHg, after which additional pressure does not yield proportional benefit. [9]
- A pilot study of class II compression stockings (23–32 mmHg) after knee arthroscopy showed significantly reduced thigh circumference at day 10 (−1.35% vs. +0.79%, p = 0.032) and significantly reduced thigh volume between days 1 and 4 (p = 0.021) compared to no compression. [10]
DVT Prevention — A Secondary Benefit
Graded compression stockings after TKA have demonstrated benefit for DVT prevention:
- Wu et al. (2025) — A retrospective cohort of 660 fast-track TKA patients found that knee-length graded compression stockings significantly reduced DVT incidence (3.8% vs. 9.6%, p < 0.05). Absence of GCS was an independent risk factor for postoperative DVT on multivariate analysis. [11]
- Maradei-Pereira et al. (2022) — A unilateral intermittent pneumatic compression device (mechanical compression) on the operated leg reduced both edema and blood loss compared to enoxaparin alone, with leg circumference increasing ~1.5 cm vs. ~2 cm (p < 0.001) and ankle swelling nearly eliminated. [12]
|
Chronic Venous Disease (CVI) |
Leg Lymphedema |
Lipedema |
Orthopedic Edema |
|
Cause: Macrovascular valve failure and fluid reflux in the deep/superficial veins. |
Cause: Microvascular clearing failure and protein-rich fluid buildup in tissue spaces. |
Cause: Genetically driven adipose and loose connective tissue symmetry disorder. |
Cause: Persistent swelling after a surgery or long periods of immobility. |
|
Symmetry: Often asymmetric; worse in the leg with higher venous back-pressure however will often show up in both legs. |
Symmetry: Heavily asymmetric; typically presenting drastically worse in one specific limb. However, lymphedema from CVI will often be both legs. |
Symmetry: Strictly symmetric; both legs present identical disproportional tissue changes. Arms and legs will be disproportionate to rest of body. |
Symmetry: Will only effect the limb where surgery or dependency has occured. |
|
The Foot Test: The ankle and lower calf swell significantly as fluid pools downward. However the foot is spared. |
The Foot Test: The foot is heavily involved; presents with characteristic square-toed swelling. Pitting edema on foot and lower ankles. |
The Foot Test: The foot is entirely spared. A distinct "cuffing" effect forms strictly at the ankle. |
The Foot Test: The foot can be significantly involved based upon the type of surgery. Total Knee Replacement and any foot/ankle surgery can cause significant foot swelling. |
|
Stemmer's Sign: Negative. The skin on the top of the second toe can be easily pinched. |
Stemmer's Sign: Positive. Skin on the toe is thickened and cannot be lifted or pinched. |
Stemmer's Sign: Negative. Foot skin remains thin and fully pliable despite heavy leg mass. |
Stemmer's Sign: Sometimes Positive. Presented in the effected in limb. Particularly of Total Knee Arthroplasty (TKA) and foot/ankle surgeries. |
|
Pain and Texture: Dull ache, heaviness, and hardness (Lipodermatosclerosis) over time. Typically worsens as the day goes on. Can have hair loss and dry skin (dermatitis). |
Pain and Texture: Soft and pitting early on; brawny, fibrotic, and highly inflammatory later. |
Pain and Texture: Highly painful to the touch; tissues bruise easily and feel like small marbles. Dense, fibrotic fatty tissue. |
Pain and Texture: Typically very painful with firm, pitting edema due to inflammation and stretching of the tissue. |
|
Compression: 20-30mmHg graduated compression is very helpful to diagnose symptoms, manage swelling and prevent worsening. |
Compression: Absolutely necessary. However type of compression is incredibly variable based upon the presentation and severity. Will typically require a consultation with a qualified lymphatic practitioner. |
Compression: Low grade compression (10-15mmHg) is a good start along with "capri" style leggings to avoid stricture in skin folds and irritation. |
Compression: Very helpful both for pain reduction and achieving range of motion. Can also be used for DVT prevention. Both 20-30mmHg can be helpful along with "fuzzy wale" for acute/sensitive areas. |
|
Treatment: Evaluation by a qualified practitioner. Normally involves a diagnostic US to confirm. Can be managed by both long term conservative measures and/or endovenous ablations. |
Treatment: Evaluation by a CLT (Certified Lymphedema Therapist) and then administer all or aspects of CDT (Completed Decongestive Therapy) |
Treatment: Evaluation by both a vascular specialist and CLT is very helpful. This should occur concurrently with a medical specialists (PCP, Endocrinologist) for management of weight, hormones, and diet. Comprehensive assessment is necessary. |
Treatment: Evaluation by a vascular specialist to rule out DVT and/or venouse disease along with treatment by a therapist that understands edema and management. Compression, elevation and movement are hallmarks of treatment. |